-
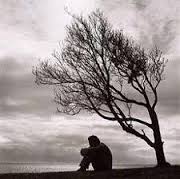
I post photos of myself smiling on Instagram but I never have a pain-free day
The truth about living with chronic pain I post photos of myself smiling on Instagram but I never have a pain-free day Lisa Harvey 5 September 2018 When was the last time you were in pain? Whatever it was – a stubbed toe, sore throat, kidney stones – chances are you recovered. Now, imagine waking up in agony most days, and knowing it probably won’t ever go away. That’s the reality for up to half of the UK’s population who live with chronic pain. And for many sufferers, life can be even more frustrating when your symptoms are often misunderstood, or worse dismissed because they’re ‘invisible’ to the naked eye.…
-
Can Tylenol Really Relieve Hurt Feelings?
Among participants who had high levels of self-reported BPD features, those in the acetaminophen group showed more trust in their partners than those who had taken a placebo. Can Tylenol Really Relieve ‘Hurt Feelings?’ Researchers say the ingredient acetaminophen can lessen extreme emotional responses, allowing people to get over rejection and other social feelings. Is it possible that Tylenol can help alleviate not just physical pain, but social pain as well? A growing body of research suggests that acetaminophen, the active ingredient in Tylenol, may help dampen emotional responses. In a study published earlier this fall, researchers from The Ohio State University found evidence that acetaminophen may reduce behavioral distrust…
-
A Horrifying Week with My Borderline Personality Disorder
I google “how to hang yourself from a radiator” in the waiting room before ducking out for a quick cry. BON: I stumbled on this over the weekend. It’s worth the time to read. It really captures the desperation of BPD. A Horrifying Week with My Borderline Personality Disorder by Heather Sleepy MENTAL ILLNESS OCT 23, 2015 I was diagnosed with Borderline Personality Disorder last December, but that was only the beginning of my troubles. This is my diary of what came after. Monday Monday is relatively chill. I manage to make it to work for 10 AM, only 30 minutes late. I’m 100 percent sure my boss thinks I’m…
-
The Death Treatment
He recently approved the euthanasia of a twenty-five-year-old woman with borderline personality disorder who did not “suffer from depression in the psychiatric sense of the word,” he said. “It was more existential; it was impossible for her to have a goal in this life.” The Death Treatment When should people with a non-terminal illness be helped to die? Letter from Belgium JUNE 22, 2015 ISSUE In her diary, Godelieva De Troyer classified her moods by color. She felt “dark gray” when she made a mistake while sewing or cooking. When her boyfriend talked too much, she moved between “very black” and “black!” She was afflicted with the worst kind of…
-
Study shows trend of prescribing opioids to patients with a comorbidity of borderline personality disorder increased over time
The results also suggest that these borderline patients may be particularly sensitive to physical pain–mirroring their well-known heightened sensitivity to emotional pain. Study shows trend of prescribing opioids to patients with a comorbidity of borderline personality disorder increased over time January 23, 2014 | By Joe Wiegel – PCLS President Patients with borderline personality disorder are being prescribed opioid pain medication at increasing rates according to a recent follow-up study by Drs. Frankenburg, Fitzmaurice and Zanarini. The researchers attempted to determine the rate of use of prescription opioid medications by patients with borderline personality disorder and compare that to the rate reported by the control group during a 10-year follow-up.…
-
Pain Really Is All In Your Head And Emotion Controls Intensity
Positive emotions — like feeling calm and safe and connected to others — can minimize pain. But negative emotions tend to have the opposite effect. Pain Really Is All In Your Head And Emotion Controls Intensity FEBRUARY 18, 2015 4:03 PM ET JON HAMILTON When you whack yourself with a hammer, it feels like the pain is in your thumb. But really it’s in your brain. That’s because our perception of pain is shaped by brain circuits that are constantly filtering the information coming from our sensory nerves, says David Linden, a professor of neuroscience at Johns Hopkins University and author of the new book Touch: The Science of Hand,…